
SEMS (Self Expandable Metal Stent) placement
Self Expandable Metal Stent is used in the treatment of defects of the gastrointestinal tract especially in perforation in the upper GI. It is a metallic tube that is used to keep the gastrointestinal track open so that food, chime, stool, and other gastric secretions can easily pass through the digestive tract. SEMS can be inserted either using the technique of endoscopy or fluoroscopy.
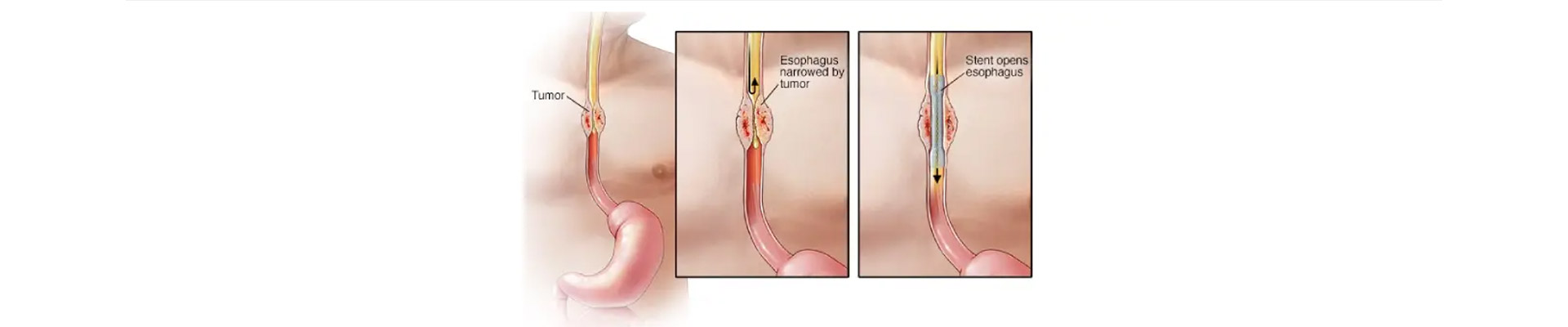
Self-expandable metal stents (SEMS) are widely accepted as a palliative treatment of Dysphagia in patients with advanced esophageal cancer. These patients are usually predicted with short-term survival. Self-expandable metal stents improve the quality of life in such patients by providing relief from dysphagia besides enhancing their nutritional and functional status. However, the procedure is associated with a risk of hemorrhage, fistula, pain, and perforation. This is one of the reasons it is not preferred to be used for patients with longer survival.
What are self-expanding metal stents made up of?
Self-expanding metal stents (SEMS) were introduced to prolong stent patency over the plastic ones. SEMS can expand 8-10 mm in diameter. They are made up of stainless steel or Nitinol which is an alloy of Nickel and Titanium. Nitinol is kink-resistant and is highly flexible. Some additional radiopaque markers are added to it to make it more radiopaque.
Which stent is better- Plastic or Metal?
Self-expanding metal stents have a longer duration of patency as compared to plastic stents, making them the right choice for all patients. However, SEMS is more costly than plastic or silicone stents. The high initial cost is one of the main reasons that has limited their use in the health care sector worldwide. Keeping the cost factor in perspective, the choice between the metal and the plastic stent depends on the survival chances of the patient.
How is SEMS deployed?
The procedure is done under sedation. The scope is passed inside to visualize the stricture. Dilation of stricture may or may not be carried out under fluoroscopy. The proximal and distal edges of the stricture are identified with the help of radiopaque markers placed under fluoroscopy. A guidewire is then placed through the scope and made to pass through the stricture. The scope is removed, the SEMS device is advanced over the wire and when it reaches the area between the two markers it is finally deployed.
Self-expanding metal stents are possible alternatives for people suffering from gastric-outlet, proximal small-bowel, and large-bowel along with esophageal obstructions. The use of SEMS is fast gaining popularity as an alternative to surgery. As these stents are deployed using endoscopy, it is less invasive than surgery and requires a shorter length of stay. Also, there are fewer chances of surgical emergencies associated with high morbidity.
SEMS are sometimes also used for placement in CBD in advance stage cancer of Gall Bladder and Common bile duct and CA head of Pancreas.
